Kinetic Compensations due to Chronic
Ankle Instability during Landing and Jumping
Ankle Instability during Landing and Jumping
Kim H, Jun
Son S, Seely MK, Hopkins JT. Medicine & Science in Sports & Exercise.
2018; 50(2): 308-317. doi: 10.1249/MSS.0000000000001442
Son S, Seely MK, Hopkins JT. Medicine & Science in Sports & Exercise.
2018; 50(2): 308-317. doi: 10.1249/MSS.0000000000001442
Take
Home Message: Those with chronic ankle instability employ
a hip-dominant strategy during jumping and landing tasks compared with healthy
individuals. The strategy may contribute to injury risk and altered performance.
Home Message: Those with chronic ankle instability employ
a hip-dominant strategy during jumping and landing tasks compared with healthy
individuals. The strategy may contribute to injury risk and altered performance.
There is
increasing information that people with chronic ankle instability (CAI) have
altered movement patterns during dynamic tasks; however, less is known about
how joints throughout the kinetic chain
may contribute to recurrent problems seen in this population. Thus, the authors
conducted a large-scale study looking at hip, knee, and ankle biomechanics in
100 individuals with CAI compared to matched healthy counterparts during a
jumping and landing task. Participants were set up in a motion capture system
and provided 5 minutes to walk on a treadmill to warm up. They were then given
up to 10 practice trials followed by 10 collected trials of a jumping and
landing protocol. This task consisted of a double leg maximum vertical forward
jump, single leg landing with the involved (and matched for healthy subjects)
limb onto a designated “x” on a force plate, immediately followed by a 90
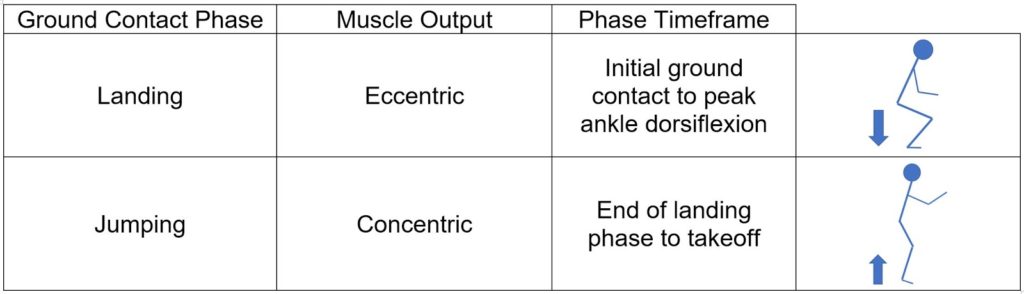
degrees side-cutting jump to the opposite side. The investigators specifically examined
data from when the foot was in contact with the ground with landing and jumping
sub-phases (see table below). The researchers compared groups based on joint power, sagittal plane jointstiffness, and joints moments.
Compared to the healthy group, the CAI group demonstrated decreased ankle and
knee 1) plantarflexion and knee extension moments during landing, 2) joint
stiffness, and 3) eccentric and concentric power during landing and early
jumping phases. Conversely, those with CAI had increased hip 1) extension
moments during landing and jumping, 2) eccentric power during early landing, 3)
concentric power during jumping, and 4) joint stiffness.
increasing information that people with chronic ankle instability (CAI) have
altered movement patterns during dynamic tasks; however, less is known about
how joints throughout the kinetic chain
may contribute to recurrent problems seen in this population. Thus, the authors
conducted a large-scale study looking at hip, knee, and ankle biomechanics in
100 individuals with CAI compared to matched healthy counterparts during a
jumping and landing task. Participants were set up in a motion capture system
and provided 5 minutes to walk on a treadmill to warm up. They were then given
up to 10 practice trials followed by 10 collected trials of a jumping and
landing protocol. This task consisted of a double leg maximum vertical forward
jump, single leg landing with the involved (and matched for healthy subjects)
limb onto a designated “x” on a force plate, immediately followed by a 90
degrees side-cutting jump to the opposite side. The investigators specifically examined
data from when the foot was in contact with the ground with landing and jumping
sub-phases (see table below). The researchers compared groups based on joint power, sagittal plane jointstiffness, and joints moments.
Compared to the healthy group, the CAI group demonstrated decreased ankle and
knee 1) plantarflexion and knee extension moments during landing, 2) joint
stiffness, and 3) eccentric and concentric power during landing and early
jumping phases. Conversely, those with CAI had increased hip 1) extension
moments during landing and jumping, 2) eccentric power during early landing, 3)
concentric power during jumping, and 4) joint stiffness.
These
findings are important because they reflect that individuals with CAI are
compensating at the hip during loaded, dynamic tasks potentially due to
limitations at the ankle. This redistribution of force may be a detrimental strategy
because it could lead to decrements in performance and heightened injury risk. These
findings highlight the need for clinicians to consider the full lower extremity
when treating individuals with CAI. The authors also recommend that these
patients may benefit from movement-related functional rehabilitation that
challenge proprioception and motor control systems. The authors acknowledged
that these findings are limited to those with CAI and cannot be extrapolated to
individuals with acute ankle sprains nor to those that are considered “copers”.
However, these findings remind clinicians to target movement patterns among
those with CAI to improve performance and mitigate the risk of injury.
findings are important because they reflect that individuals with CAI are
compensating at the hip during loaded, dynamic tasks potentially due to
limitations at the ankle. This redistribution of force may be a detrimental strategy
because it could lead to decrements in performance and heightened injury risk. These
findings highlight the need for clinicians to consider the full lower extremity
when treating individuals with CAI. The authors also recommend that these
patients may benefit from movement-related functional rehabilitation that
challenge proprioception and motor control systems. The authors acknowledged
that these findings are limited to those with CAI and cannot be extrapolated to
individuals with acute ankle sprains nor to those that are considered “copers”.
However, these findings remind clinicians to target movement patterns among
those with CAI to improve performance and mitigate the risk of injury.
Questions
for Discussion: What rehabilitation protocols have
others implemented to target full lower extremity movement patterns? What are
other functional movements that would be important to assess as they pertain to
injury risk and performance?
for Discussion: What rehabilitation protocols have
others implemented to target full lower extremity movement patterns? What are
other functional movements that would be important to assess as they pertain to
injury risk and performance?
Written by: Alexandra F. DeJong
Reviewed by:
Jeffrey Driban
Jeffrey Driban
Related Posts:
