As promised here is Part II of Evaluating the Scapula. Enjoy!!
W. Ben Kibler, MD
Aaron Sciascia, MS, ATC, NASM-PES
Shoulder Center of Kentucky
Posture and Flexibility
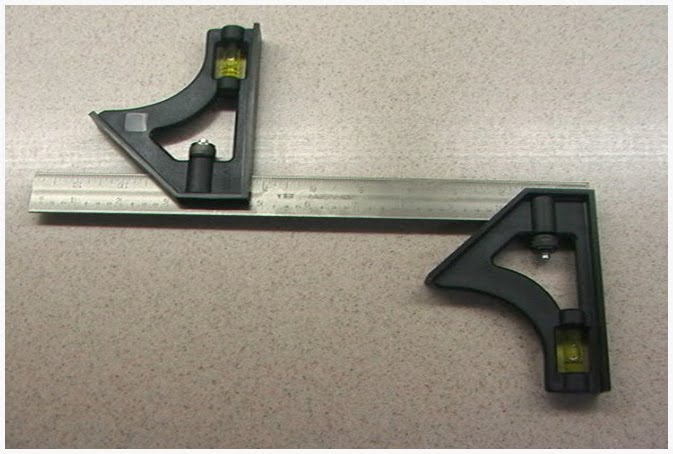
Coracoid based inflexibility can be assessed by palpation of the pectoralis minor and the short head of the biceps brachii at their insertion on the coracoid tip. They will usually be tender to palpation (even if they are not symptomatic in use), can be traced to their insertions as taut bands, and will create symptoms of soreness and stiffness when the scapulae are manually maximally retracted and the arm is slightly abducted to approximately 40-50 degrees. A rough measurement of pectoralis minor tightness may be obtained by standing the patient against the wall and measuring the distance from the wall to the anterior acromial tip. This can be done using a “double square” device with a patient standing with his or her back against a wall (Figure 3). A bilateral measurement is taken (in inches or centimeters) to determine if there is a notable difference between the involved and non-involved shoulder.
 To obtain accurate internal rotation measurements from the shoulder, place the patient supine on a flat level surface. It is beneficial to have a second examiner positioned behind the athlete in order to properly stabilize the scapula to ensure that scapular movement does not occur. The humerus is supported on the surface with the elbow placed at 90° and the arm on a bolster in the plane of the scapula. The clinician passively moves the arm into internal rotation obtaining the measurement using a goniometer or inclinometer following standard alignment procedures. Rotation is taken to “tightness”, a point where no more GH motion would occur unless the scapula would move. This measurement should be taken bilaterally.
To obtain accurate internal rotation measurements from the shoulder, place the patient supine on a flat level surface. It is beneficial to have a second examiner positioned behind the athlete in order to properly stabilize the scapula to ensure that scapular movement does not occur. The humerus is supported on the surface with the elbow placed at 90° and the arm on a bolster in the plane of the scapula. The clinician passively moves the arm into internal rotation obtaining the measurement using a goniometer or inclinometer following standard alignment procedures. Rotation is taken to “tightness”, a point where no more GH motion would occur unless the scapula would move. This measurement should be taken bilaterally.
Horizontal adduction measurements are helpful in determining if posterior shoulder tightness is present. Passive glenohumeral horizontal adduction is measured with the patient supine and the shoulder and elbow in 90o of abduction and flexion respectively. The clinician stabilizes the scapula at the lateral border and then horizontally adducts the humerus to the point of pain or end range of glenohumeral motion.
Symptom Alteration (Corrective Maneuvers)
If scapular dyskinesis is demonstrated on the clinical exam of patients with shoulder injury, different types of corrective maneuvers may be employed to determine the effect of the altered motion on symptoms or signs of shoulder injury. The goal of the maneuvers would be to alter or reduce some of the signs or symptoms.
The scapular assistance test (SAT) and scapular retraction test (SRT) are corrective maneuvers that may alter the injury symptoms and provide information about the role of scapular dyskinesis in the total picture of dysfunction that accompanies shoulder injury and needs to be restored. The SAT helps evaluate scapular contributions to impingement and rotator cuff strength, and the SRT evaluates contributions to rotator cuff strength and labral symptoms. In the SAT, the examiner applies gentle pressure to assist scapular upward rotation and posterior tilt as the patient elevates the arm (Figure 4). A positive result occurs when the painful arc of impingement symptoms is relieved and the arc of motion is increased.
In the SRT, the examiner grades the supraspinatus muscle strength following standard manual muscle testing procedures (or by a hand held dynamometer). The clinician then manually places and stabilizes the scapula in a retracted position (Figure 5). A positive test occurs when the demonstrated supraspinatus strength is increased or the symptoms of internal impingement in the labral injury are relieved in the retracted position.
Although these tests are not capable of diagnosing a specific form of shoulder pathology, a positive SAT or SRT shows that scapular dyskinesis is directly involved in producing the symptoms and indicates the need for inclusion of early scapular rehabilitation exercises to improve scapular control.
In closing, we would like to thank Dr. Ben Kibler and Aaron Sciascia for putting together a great comprehensive guide for evaluating the scapula. They both have very busy schedules and we are very grateful for them taking the time to do this.