Reliability and validity of
three pain provocation tests used for the diagnosis of chronic proximal
hamstring tendinopathy
three pain provocation tests used for the diagnosis of chronic proximal
hamstring tendinopathy
Cacchio
A., Borra F., Severini G., Foglia A., Musarra F., Taddio N., De Paulis F.
A., Borra F., Severini G., Foglia A., Musarra F., Taddio N., De Paulis F.
British
Journal of Sports Medicine. 2012; 46:883-887.
Journal of Sports Medicine. 2012; 46:883-887.
Proximal hamstring
tendinopathy is an overuse injury and the main symptom is typically an ill-defined
pain during activity in the area of the ischial tuberosity. Due to injuries
with similar symptoms (e.g., piriformis syndrome) it is difficult to correctly
diagnose proximal hamstring tendinopathy. Therefore, the objective of this study
was to assess the reliability and validity as well as the sensitivity and
specificity of 3 pain provocation tests for the diagnosis of proximal hamstring
tendinopathy. Ninety-two professional athletes with (n = 46) and without (n =
46) proximal hamstring tendinopathy were included in this study. All the
athletes underwent a clinical examination of the pelvic, hip, and back region.
After that, the athlete’s history was taken. A positive diagnosis of proximal
hamstring tendinopathy was made by an expert physician when an athlete had pain
in the lower gluteal region (visual analog scale score of ≥ 4 cm), tenderness
at the ischial tuberosity (mild to considerable pain), and positive findings on
magnetic resonance imaging. Three physiotherapists performed the three pain
provocation tests after being trained to perform the tests by a physician. The Puranene-Orava test required the patients to stretch their own hamstring muscles in a
standing position with the hip at 90 degrees and the knee fully extended with the
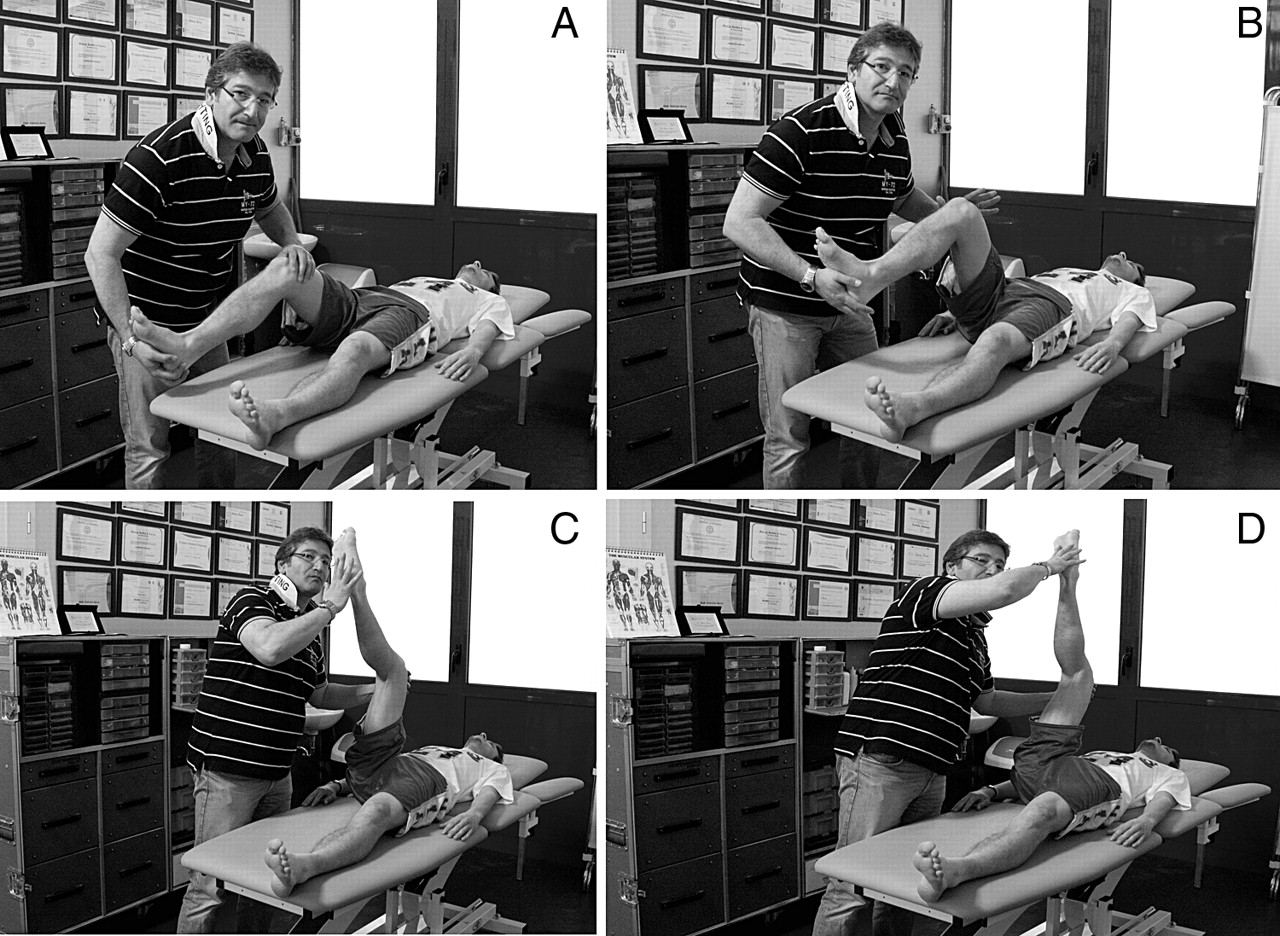
foot on a support. The second pain test was the bent-knee stretch which
required the patients to lay supine while the examiner maximally flexed the
patient’s hip and knee of the symptomatic leg and then slowly straightened the
knee. The third pain test was the modified bent-knee stretch that required the patients to lay supine with their legs fully
extended. The examiner then maximally flexed the hip and knee of the
symptomatic leg and finally rapidly extends the knee. All three tests were
assessed based on a 4-point pain scale (no pain to unbearable pain). The three
physiotherapists were blinded to whether the patients were diagnosed with
proximal hamstring tendinopathy. The physiotherapists independently performed
the exams bilaterally with each test randomized (all exams were performed
within a 30 minute session). Among 35 participants, two examiners performed a
second evaluation 3 days later at the same time of the day as the previous test
with no therapy in between. Inter-examiner and intra-examiner reliability were
good for both symptomatic and asymptomatic patients. The Puranene-Orava test
had high sensitivity and specificity along
with a positive predictive value (PPV, true positive findings divided by all positive findings
with test) of 81%, and a negative predictive value (NPV, true negative findings divided by all negative findings
with the test) of 77%. The bent-knee stretch had a high sensitivity and
specificity with a PPV of 86%, and a NPV of 85%. The modified bent-knee stretch
also had a high sensitivity and specificity with a PPV of 91%, and a NPV of
89%.
tendinopathy is an overuse injury and the main symptom is typically an ill-defined
pain during activity in the area of the ischial tuberosity. Due to injuries
with similar symptoms (e.g., piriformis syndrome) it is difficult to correctly
diagnose proximal hamstring tendinopathy. Therefore, the objective of this study
was to assess the reliability and validity as well as the sensitivity and
specificity of 3 pain provocation tests for the diagnosis of proximal hamstring
tendinopathy. Ninety-two professional athletes with (n = 46) and without (n =
46) proximal hamstring tendinopathy were included in this study. All the
athletes underwent a clinical examination of the pelvic, hip, and back region.
After that, the athlete’s history was taken. A positive diagnosis of proximal
hamstring tendinopathy was made by an expert physician when an athlete had pain
in the lower gluteal region (visual analog scale score of ≥ 4 cm), tenderness
at the ischial tuberosity (mild to considerable pain), and positive findings on
magnetic resonance imaging. Three physiotherapists performed the three pain
provocation tests after being trained to perform the tests by a physician. The Puranene-Orava test required the patients to stretch their own hamstring muscles in a
{kind=link}
standing position with the hip at 90 degrees and the knee fully extended with the
foot on a support. The second pain test was the bent-knee stretch which
required the patients to lay supine while the examiner maximally flexed the
patient’s hip and knee of the symptomatic leg and then slowly straightened the
knee. The third pain test was the modified bent-knee stretch that required the patients to lay supine with their legs fully
{kind=link}
extended. The examiner then maximally flexed the hip and knee of the
symptomatic leg and finally rapidly extends the knee. All three tests were
assessed based on a 4-point pain scale (no pain to unbearable pain). The three
physiotherapists were blinded to whether the patients were diagnosed with
proximal hamstring tendinopathy. The physiotherapists independently performed
the exams bilaterally with each test randomized (all exams were performed
within a 30 minute session). Among 35 participants, two examiners performed a
second evaluation 3 days later at the same time of the day as the previous test
with no therapy in between. Inter-examiner and intra-examiner reliability were
good for both symptomatic and asymptomatic patients. The Puranene-Orava test
had high sensitivity and specificity along
with a positive predictive value (PPV, true positive findings divided by all positive findings
with test) of 81%, and a negative predictive value (NPV, true negative findings divided by all negative findings
with the test) of 77%. The bent-knee stretch had a high sensitivity and
specificity with a PPV of 86%, and a NPV of 85%. The modified bent-knee stretch
also had a high sensitivity and specificity with a PPV of 91%, and a NPV of
89%.
Based on the reliability and
validity calculations for the Puranene-Orava, bent-knee stretch, and modified
bent-knee stretch we can infer that they may be good tests to assess proximal
hamstring tendinopathy. All 3 tests must be easy to perform since both the
inter-examiner and intra-examiner reliability (repeatability) scores were high
to very high, respectively. The 3 tests seem to have moderate-to-good levels of
diagnostic validity. The least accurate test was the Puranene-Orava. This may
be due to the test being performed by the patient and that the patient may stop
the test early due to pain. The most accurate test was the modified bent-knee
stretch, which may elicit a greater pain response due to the examiner rapidly extending
the knee. The authors suggest that these tests are not strong enough to make a
clinical diagnosis alone and that they should be used in conjunction with magnetic
resonance imaging. Have you calculated inter-examiner or intra-rater
reliability at your clinics for repeatability and consistency? Do you have any
experience with these three tests? What diagnostic tests do you use to assess
proximal hamstring tendinopathy?
validity calculations for the Puranene-Orava, bent-knee stretch, and modified
bent-knee stretch we can infer that they may be good tests to assess proximal
hamstring tendinopathy. All 3 tests must be easy to perform since both the
inter-examiner and intra-examiner reliability (repeatability) scores were high
to very high, respectively. The 3 tests seem to have moderate-to-good levels of
diagnostic validity. The least accurate test was the Puranene-Orava. This may
be due to the test being performed by the patient and that the patient may stop
the test early due to pain. The most accurate test was the modified bent-knee
stretch, which may elicit a greater pain response due to the examiner rapidly extending
the knee. The authors suggest that these tests are not strong enough to make a
clinical diagnosis alone and that they should be used in conjunction with magnetic
resonance imaging. Have you calculated inter-examiner or intra-rater
reliability at your clinics for repeatability and consistency? Do you have any
experience with these three tests? What diagnostic tests do you use to assess
proximal hamstring tendinopathy?
Written
by: Jane McDevitt MS, ATC, CSCS
by: Jane McDevitt MS, ATC, CSCS
Reviewed
by: Jeffrey Driban
by: Jeffrey Driban
Related
Posts:
Posts:
Cacchio A, Borra F, Severini G, Foglia A, Musarra F, Taddio N, & De Paulis F (2012). Reliability and validity of three pain provocation tests used for the diagnosis of chronic proximal hamstring tendinopathy. British Journal of Sports Medicine, 46 (12), 883-7 PMID: 22219215